

Maximiliano Escobar
'And if I must love you at this new distance, I will love you so fiercely it will be felt in every universe that lies between us.'
Sara Rian
Maxi's Journey
Maxi was born full-term at 39+3 after an amazing pregnancy with no issues at all. His anatomy scan looked great, his genetic testing was low-risk for everything, and he entered the world as fast as can be. I arrived at the hospital at 8cm dilated at 8.45pm & in 1 euphoric push, Maxi was born at 9.52pm. He didn't really let out that loud, clear, baby cry. He sounded very crackly and congested and the nurses deep suctioned him, but were a little confused because nothing really came out. They told me he had inhaled quite a bit of amniotic fluid and that this must be why he sounded so congested and coarse—but little did we know, that was the first sign of the cleft.
They left him on my chest for about two hours while we snuggled. I attempted to latch him; he latched for a very short time and just seemed very tired, but I didn’t think anything of it besides him being a sleepy, noisy little newborn. When the nurses came back in and took him to check on him, they told me he was a bit cold and needed to be warmed up in the nursery and that they’d bring him right back. When I went to check on him, they fed him some of my colostrum, which he drank, but his breathing rate increased a lot, and I didn’t like the way his chest was retracting. They requested chest X-rays. Once the pediatrician reviewed them and spoke to us, he explained that I’d had a precipitous labor, which meant Maxi didn’t squeeze out all of the fluid on the way out, and the X-ray of his chest looked extremely wet because of this. He said that Maxi needed to do something in the sense of clear his throat, but because he was a baby, he didn’t know how to do that.
At 15 hours, they admitted him to the NICU, where he needed extra respiratory support, and they told me they would begin antibiotics for what was presenting as pneumonia. They said that once the antibiotics were complete, which would be about seven days, we could go home.
They inserted a feeding tube down his mouth and told us we could attempt to orally feed once his breathing rate was steadily between 40 and 60bpm and once he was down to 2 liters of oxygen. Unfortunately, it never got there, and Maxi was on full CPAP by day 7 due to episodes of throwing up. He always had so many secretions, but the doctor said the CPAP was pumping his tummy full of air and there was no space for his lungs to inhale, which was why he was throwing up.
He wasn’t making the progress we needed to see, so the doctor told me they would order an ENT consult. The ENT consult came back clear, so the next step was a swallow study. The doctor told me the worst-case scenario could be a fistula, but they didn’t believe that was the case because they had been able to pass a feeding tube, and usually babies with fistulas aren’t able to breathe as well as he was. I didn’t even look into fistulas at that point—I suppose the doctors telling me it was unlikely made me not worry about it.
His swallow study showed immediate aspiration, and the X-ray showed a clear connection between the trachea and esophagus, which they called an H-type fistula. I was devastated because I knew this meant he needed surgery, and it killed me to know my little baby needed to be cut open. But I was relieved, in a way, that we finally knew what it was and that this meant we were closer to going home. I spoke with the pediatric surgeon, who said this was a better type of fistula to have because at least his esophagus was connected to his stomach. In preparation for surgery, he had an echo, which came back perfectly fine, and ultrasounds of his kidneys and brain, which both also came back clear.
Maxi went in for surgery, and 15 minutes later the surgeon was walking toward us visibly shaken, and my heart sank. He showed us the pictures from the bronchoscopy, but we had no idea what we were looking at, and he couldn’t explain it to us in that moment. He simply said he could not do the surgery because it would be fatal for Maxi, and that he needed to stay in the hospital and grow to 16 pounds. It took us some time to process the news, and even later I still didn’t fully understand what his diagnosis was. I requested to speak to a doctor since I never saw the surgeon again, and the doctor on call told me it was a type 4 laryngeal cleft. She explained it as the esophagus and trachea being fused together & said they had never seen it before.
I was able to speak with the chief pediatric ENT surgeon at another hospital in San Antonio, Texas, and he told me that no team in San Antonio had adequate experience with a type 4 cleft. He said our best option would be to transfer to Texas Children’s in Houston. He gave me the direct phone number for the Aerodigestive Team Medical Director, Dr. Deepak Mehta, and explained that it wasn’t just a good surgeon we needed—we needed a good institution as well. I didn’t fully understand what he meant at the time, but I did once we arrived at Texas Children’s.
We ended up transferring to Texas Children’s Hospital in Austin, which was their newest location and such a relief because it was much closer to us, 200 miles away but still closer than Houston. We were picked up by the Kangaroo Crew in San Antonio, transferred directly to the PICU, and greeted with a warm, reassuring welcome. I felt an instant relief—we were finally in the right place with people who had experience and truly knew what they were doing. We were immediately met by a team of doctors and pediatric surgeons waiting for us. The pediatric ENT whose specialty was complex airway disorders came in right away to meet us. His name was Dr. Scott Schraff. Dr. Mehta and Dr. Schraff were colleagues, and both had completed their residency at Cincinnati Children’s Hospital, working directly with Dr. Rutter, who is known as the top surgeon for complex laryngeal clefts. This gave me even more peace of mind that my son was in good hands.
Dr. Schraff rolled in a whiteboard, drew diagrams, and explained everything to us in detail. He also explained the surgery thoroughly. He told us that he and another pediatric surgeon, Dr. Matias Bruzoni, would be performing the surgery together. They would be opening Maxi’s chest, and Maxi would have to be on bypass—something I had never heard of before, but quickly learned about, and it terrified me more than anything. He also told us that after surgery, Maxi would most likely need a trach for a few years, but it should be removed by kindergarten. All of this was extremely frightening to hear, but I was still relieved to finally be talking to someone who understood exactly what they were dealing with and who was confident in their abilities.
He was very surprised that Maxi didn’t have any other known anomalies at that point and also surprised that he was on such minimal respiratory support. He actually did not believe Maxi had a type 4 cleft. After examining him, he felt it might be something involving Maxi’s vocal cords, but when he checked with a mini scope, his vocal cords looked perfectly fine. We would find out soon enough, since they planned to do their own tests and take him to the OR the following week for a bronchoscopy.
They performed extensive CT scans, and one of the pediatric surgeons told me they were able to get very good imaging. The scans showed that the cleft was not as severe as originally thought, which meant he would not need to be on bypass for surgery. This was the best news I could have received at that time.
To Dr Schraff’s surprise, the bronchoscopy confirmed that Maxi did indeed have a type 4 laryngeal cleft—but it was considered a ‘better’ scenario for a type 4 because it was 3 cm above the carina. Again, I had no idea what a carina even was at the time, but I learned so much throughout this journey. They told us they would prepare for surgery in the next three days. The night before his surgery, I received a late phone call from Dr. Schraff explaining that they had just finished a conference call with Dr. Rutter in Cincinnati, Dr. Deepak Mehta in Houston, and Dr. Bruzoni to discuss Maxi’s case. He told me that since Maxi was doing very well for a baby with a type 4 laryngeal cleft, had no other known anomalies, and had a healthy heart, the best option—for him to survive the surgery and have the best long-term outcome—was to wait until he was at least 5 kg. This recommendation was based on data from Cincinnati Children’s Hospital and their long history with type 4 laryngeal clefts. Maxi was barely 3 kg at this point, and it took us some time to process what this would mean. But once we heard the phrase “best long-term outcome for him,” we immediately agreed.
We made all the necessary arrangements now that we would essentially be living in two cities while raising a three-year-old toddler. It was extremely hard and we were in complete survival mode but we made it work somehow. Up until this point, I had been very hesitant to join any laryngeal cleft groups on Facebook. I had already been through so much, and I didn’t know what to expect from other people’s stories—what I would read, or what I would hear. But at this stage, I took a leap and joined the laryngeal cleft groups. I reached out to the Laryngeal Cleft Network, where I spoke with Carolyn, and I connected with parents of other type 4 kiddos to hear their stories and get even the slightest glimpse into their lives. I’m not going to lie—I was terrified reading and hearing about what other type 4 children had been through. And the fact that there were so few of them really hit me just how rare this disorder truly is. While it was frightening, it was also extremely helpful to have some idea of what to expect, even though Maxi wasn’t very comparable to any of the other type 4s. Each kiddo truly is unique. But I knew I wasn’t alone and that I had resources which was a comfort.
We spent the next few months in the hospital growing and having daily weigh-ins. That came with its own set of challenges. Maxi had a G-tube placed but he was unable to tolerate feedings directly into his stomach through the G-tube. So an interventional radiologist placed an NG tube that bypassed his stomach and fed directly into his small intestine, and he remained on continuous fortified high calorie feeds. He was able to be completely weaned off oxygen, which was a huge win for us. His surgeon told us he had a strong respiratory drive, which would be incredibly helpful post-surgery and might even mean he could get through surgery without needing a trach. He was doing so well that they discharged him from PICU and transferred him to acute care.
I wasn’t happy about the transfer to acute care. It meant fewer eyes on him, and my biggest concern was that if something happened—especially vomiting and aspirating—he would need immediate attention. Well, it ended up being an unfortunate blessing in disguise. The very afternoon I was with Maxi in acute care, he had an episode of vomiting, and his vitals took a significant hit. We were transferred back to the PICU, where we stayed until surgery.
Maxi’s weight gain was very slow. Some days he would gain, other days he would lose, despite having fortified breast milk and formula. We were all concerned about why he was losing weight and how it would affect the surgery timeline. Dr. Schraff consulted again with Dr. Rutter and Dr. Mehta about our situation, and they advised that since Maxi was off respiratory support, his work of breathing was much harder because of the cleft, even though his vitals always looked good. He was burning calories like crazy just by breathing, so they made the decision to keep him on 7 liters of high-flow support. Once we did that, we finally saw consistent weight gain, which was a huge relief.
Maxi's surgery was scheduled for December 16th. The PICU nurses prepared me so well on what post-recovery surgery would look like and how he would have a breathing tube in and how we would manage it. I was very disheartened that he was going to have a breathing tube in and be recovering from surgery over Christmas, but at the same time we also really just wanted to be one step closer to getting him home. Two days before his scheduled surgery, they called me late at night and told me he had just spiked a fever and tested positive for rhinovirus. The surgeons contacted me and let me know that his surgery would be postponed for at least three weeks, but it would probably be a better option, as he wasn't quite 5kg yet and over Christmas, the hospital is not as fully staffed as usual, and it would end up working out for the best. I was honestly so relieved, and it turned out to be the biggest blessing for our family, because in those three weeks Maxi thrived so much in his growth and in his milestones, and because it was the holidays, we got to spend time together as a whole family. We made the the absolute most of spending Christmas and New Year's in a hospital and we even got to take Maxi on his first walk outside on Christmas Day. I will forever cherish the beautiful memories that we have from this time.
Maxi reached 6 kg on the day of his surgery on January 13th. He was big and strong and I finally felt like he was ready and so was I.
Dr. Mehta traveled down from Houston for the surgery, and I was told that the gallery was full because so many people wanted to observe such a rare procedure. The pediatric plastic surgeon informed us that they planned to take a graft from Maxi’s leg to place it between his esophagus and trachea. After the bronchoscopy, Dr. Schraff and Dr. Bruzoni came out to show us pictures of his airway. They were very happy with what they saw, and we were officially cleared for surgery.
The surgery lasted about seven hours. They were able to go through his neck, and everything went very well. They didn’t end up needing a graft from his leg—they were able to take a good piece from his chest instead. Dr. Schraff said Maxi’s lungs looked surprisingly good despite all the aspiration he had experienced. He also said Maxi would not need to be kept paralyzed during recovery and that the breathing tube would remain in for at least 10 days before they returned to the OR for a post-op bronchoscopy to evaluate his airway and see if they could extubate him. (Continued below)
Continued ~Journey
Post-surgery recovery was extremely brutal—probably more brutal for me. Maxi got so strong while he grew, he was rolling before his surgery and meeting all his milestones so he wanted to be active and moving but he wasn’t allowed to whip his head back and forth so he unfortunately was given a cocktail of narcotics to keep him pretty sedated and asleep. He ended up becoming delirious from the narcotics, and for a couple of very hard days, the nurses, respiratory therapists, and I worked nonstop to keep his breathing tube in place and prevent his head from hyperextending. This took such a heavy toll on me in every way, watching Maxi continuously getting sedated, not being able to hold him, seeing him struggle with the delirium
After 10 days, he went back to the OR. They successfully removed the breathing tube and returned him to the PICU on CPAP. Unfortunately, once he began waking up, he developed major chest retractions, and it became clear that breathing was just too difficult for him. He was re-intubated, and it was confirmed that he would need a trach. I was heartbroken, seeing him breathe so hard and I had high hopes we possibly wouldn’t need the trach because of how well he had always done. They scheduled him for a tracheostomy and a Nissen fundoplication to address his severe reflux and make sure he could safely be fed through his G-tube at home.
Both of those procedures went well. He remained on very low ventilator settings post op and Dr. Schraff was eager and confident that Maxi could eventually be weaned off the ventilator. Eight days after his tracheostomy, he had his first HME filter trial for 30 minutes. Maxi did so well that they increased his time day by day until he was on HME’s during the day and using the ventilator only at night for pressure support. He never needed oxygen from the ventilator, which was a huge win for us.
He began speech therapy, and that’s when I learned about the speaking valve. We were able to trial it, and he did great with that too. Everyone was consistently surprised and impressed by Maxi and his progress, and it gave us so much hope for his future.
We were completely committed to learning everything we needed to know to become medical parents and to finding the best therapists and medical team for him in San Antonio. As we prepared for discharge, the pulmonologist was surprised by how well Maxi breathed on HME’s. She had done her own bedside scope and said his tracheomalacia was more severe than he appeared to show. She increased his pressure support on the ventilator for nighttime and sick settings, and we left the hospital using HME’s during the day and the ventilator at night.
When we were doing the simulations of worst-case scenarios—practicing CPR and preparing for emergencies—we felt a small sense of relief. The nurses and RTs told us that because Maxi didn’t need oxygen, if we ever had to take him to the hospital, it likely wouldn’t be in an extreme emergency. I wish those words had turned out to be true.
Maxi spent four nights at home before he suddenly stopped breathing and had to be rushed to the hospital. It was unexpected, devastating, and a harsh reality of the severity of his struggle being born with this type of airway disorder. Maxi didn’t make it, and he passed away in our arms on March 7th, 2025.
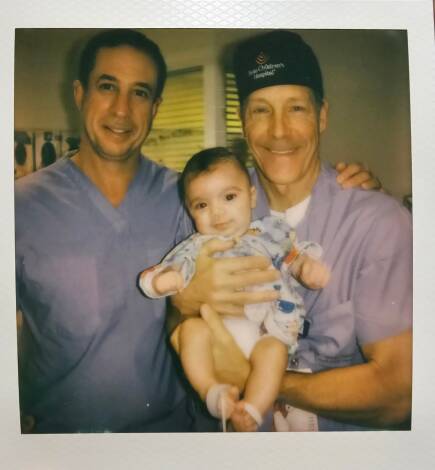
I always imagined writing his story someday, but not like this. I imagined writing it for him—so he could read it when he was older, feel proud of the mighty fight he fought, and know what a little warrior he was. I documented his entire journey taking pictures with his entire care team to show him one day. He was so deeply loved and adored at Texas Children’s. They became our second family, and everyone was so invested in his care and always rooting for him. I am so incredibly proud of him, and even prouder to be his mother.
His life & his journey broke me, humbled me, strengthened me and healed me all at once. He is and forever will be my greatest gift, and his life will forever be remembered, honored, and cherished with all of our hearts.
In loving memory ~ Maximiliano Armando Escobar
09/12/2024 – 03/07/2025
Gallery
























Memory wall
Maxi’s story helped me through the loss of my laryngeal cleft baby all the way here in Australia. His journey will also help others, thank you for sharing such a difficult time in your life. 💛
I would call you sunshine when you smiled at me, because that’s exactly what you are…pure, radiant sunshine.







 Français
Français Deutsch
Deutsch Nederlands
Nederlands Español
Español Português
Português Magyar
Magyar Русский
Русский 繁體中文
繁體中文